
What is the Problem AMHC Addresses?
 Motor vehicle (MV) injury remains THE leading cause of death and serious injury among New Zealand adolescents age 15-19. New Zealand also has the highest adolescent road crash death rate among OECD countries. Young Australians have a road fatality rate of 13 while young New Zealanders have a fatality rate of 21 per 100,000 population. Regrettably, NZ adolescents are no more safe than they were 10 years ago. Maori youth are at substantially increased risk for both motor vehicle mortality and serious injury.
Motor vehicle (MV) injury remains THE leading cause of death and serious injury among New Zealand adolescents age 15-19. New Zealand also has the highest adolescent road crash death rate among OECD countries. Young Australians have a road fatality rate of 13 while young New Zealanders have a fatality rate of 21 per 100,000 population. Regrettably, NZ adolescents are no more safe than they were 10 years ago. Maori youth are at substantially increased risk for both motor vehicle mortality and serious injury.
But other harms from car use, outside the gaze of injury prevention and driver education programmes, go far beyond traffic injuries. Although poorly documented, ‘non-traffic’ teen risks from car use include physical inactivity, obesity, alcohol and drug use, poorer grades, and sexually transmitted diseases. In addition, ubiquitous driving places huge external costs on society in the forms of noise, pollution, congestion, sprawl, community severance, inequity, energy poverty, energy depletion, biosphere harm and climate change.
There has been some progress. This has been mainly due to graduated driver licensing (GDL) policies that have reduced exposure to unsupervised driving during the training period and recently, by raising the minimum driving age. This suggests that for many youth reducing exposure to car use is an under-tapped strategy to reduce the ongoing burden of adolescent MV injury.
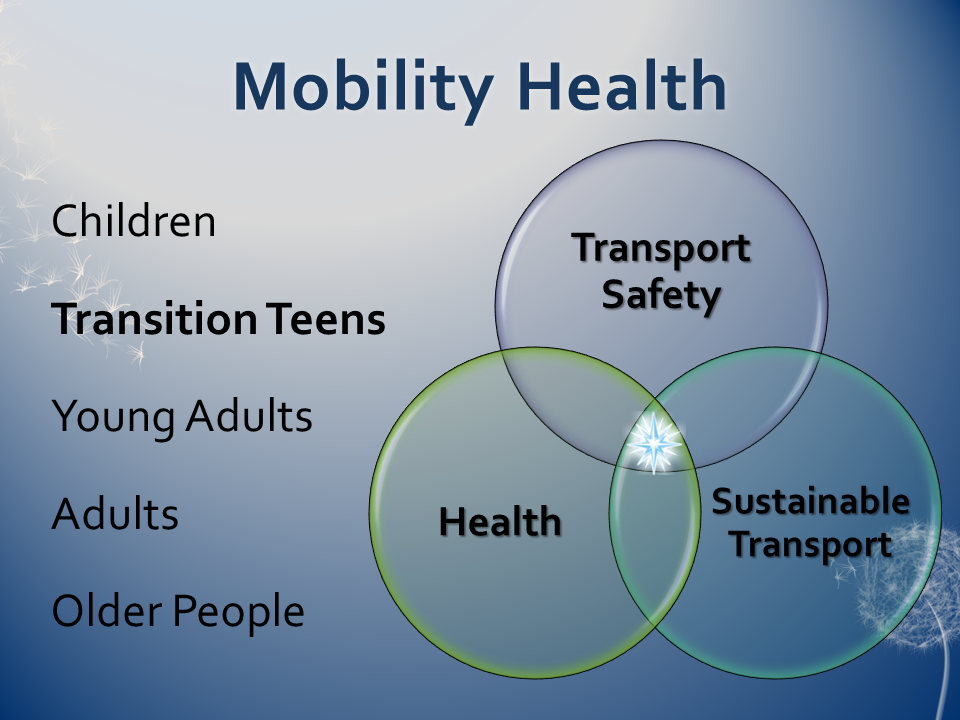
We advocate changing the current narrow paradigm of adolescent road safety that focuses mainly on crash risk, to the broader, more potent, timely and healthy vision of less driving through mobility modal shift from cars to active and public transport. We have named this paradigm shift “mobility health”. This area represents the intersection and dynamics of considering simultaneously health and well being, transportation safety and environmental sustainability.
Why Youth?
Youth are a critical population to target mobility health strategies for many reasons:
- As shown above they are a very high risk group for crashes and injury.
- However, efforts to address this have plateaued out in many developed countries and youth driver education has not been very effective.
- Because many of the victims of teen crashes are occupants of other vehicles, reducing teen crashes has a large beneficial multiplier effect on all road users.
- They lack strong status quo bias compared to older adults and may be less likely to exhibit cognitive dissonance. Most youth do not own a car and younger youth are still non-drivers. Therefore, they have not yet formed car-use or car dependent habits as drivers (though they may have as passengers), which might otherwise make them more resistant to change.
- Adolescents are less likely to have physical barriers to increasing active transport
- Healthy mobility habits learned at this stage may be engrained for many years.
- They are at a stage when many make decisions about whether to learn to drive, how much and how far to drive, and whether to buy a car, not just whether to drive safely. Hence, they also have the stimulus at this important juncture to consider their choices, and “may be more receptive to new ideas and information” (Cairns, 2003)”
- They may not yet have been exposed to the variety of objective information needed in order to help make the best decisions for themselves so information may be just the nudge they need.
- They may be more sensitive to cost considerations due to limited means.
- Simultaneously, they may be vulnerable to advertising glorifying the appeal of car use but ignoring the drawbacks of safety, costs, activity levels, and so on.
- Parents and peers can play a special role in influencing youth attitudes and behaviours.
- The school setting that most youth are in allows for a dynamic range of mobility health education and programs involving both teachers and students as leaders
- The generation of today’s youth are those that will very likely live long enough to experience for themselves very serious consequences of climate change (Nature Climate Change, 2011) so they have a strong personal stake in addressing the environmental issues.
Goal
The goal of the Adolescent Mobility Health Consortium (AMHC) is to encourage, develop and support research and interventions that facilitate voluntary adolescent transportation modal shift from motor vehicles to active and public transport. Many of these interventions go under the umbrella term of “transportation demand management” (TDM), also known as “mobility management” (MM).
 TDM is potentially more beneficial to adolescents than traditional road safety efforts aimed at making a costly, risky and unhealthy activity (driving) marginally safer. These efforts aim to promote the consideration and adoption of alternatives to the cultural and generational expectations of ubiquitous driving in private automobiles. It is about the freedom for youth to choose their mobility options with full knowledge of the benefits and drawbacks of each alternative.
TDM is potentially more beneficial to adolescents than traditional road safety efforts aimed at making a costly, risky and unhealthy activity (driving) marginally safer. These efforts aim to promote the consideration and adoption of alternatives to the cultural and generational expectations of ubiquitous driving in private automobiles. It is about the freedom for youth to choose their mobility options with full knowledge of the benefits and drawbacks of each alternative.
Who We Are
The AMHC builds on parallel work in the School of Medicine, the University and other entities. It draws from multiple disciplines including (but not limited to) marketing, science communication, geography, adolescent psychology, education, risk measurement, activity and wellness promotion, injury epidemiology, exposure assessment, and environmental health.
The AMHC received its initial strategic development support in July, 2011 through a planning grant from the Dunedin School of Medicine and the Southern District Health Board.
AMHC is a project within the Injury Prevention Research Unit (IPRU). IPRU is part of the Department of Preventive and Social Medicine at the Dunedin School of Medicine, University of Otago.
Comments