
Tim Chambers, Simon Hales, Jude Ball, Michael Baker, Cristina Cleghorn, Nick Wilson (*Author details)
The Climate Change Commission’s final advice to the Government has been tabled in Parliament. This final report further acknowledged the potential health co-benefits of climate action presented in the Commission’s draft advice. However, the Commission has excluded these health co-benefits from its economic analyses, which currently predict a reduction in GDP of 0.2-1.0% in 2035 and 0.3-0.7% in 2050. Thus, the Commission’s final advice inadequately accounts for the financial benefits of reduced air and water pollution, increased active transport, improved housing and improved diets that could potentially result in net long-term savings to society from responding to climate change.

Image by Luke Pilkinton-Ching, University of Otago Wellington.
The Climate Change Commission’s final advice to the Government made incremental improvements by acknowledging a broader range of evidence on the health co-benefits of climate change mitigation actions.1 However, its economic analyses fail to incorporate the economic value of these health co-benefits which could well result in net savings to society from responding to climate change. In this blog, we: 1) review the additional health co-benefits included by the Commission from its draft advice;2 2) highlight some omissions of key health co-benefits; and 3) highlight the magnitude of the potential cost-savings from the health co-benefits mentioned and omitted from the Commission’s final advice.
Our submission on the Commission’s draft advice called for greater recognition of the health co-benefits of climate action.3 Specifically, we called for greater consideration of the major opportunities for health gains from increased physical activity, improved housing, reduced air and water pollution and healthier diets. The Commission’s final advice included more NZ evidence on the health benefits and health equity implications of increased physical activity than the draft advice.4,5 One of these studies estimated the lifetime healthcare cost-savings of substituting short vehicle trips to walking and cycling could be up to $2.1 billion.4 Likewise, the Commission’s final advice added more evidence on the favourable cost-benefit ratio of improved housing,6,7 in addition to evidence presented in the draft advice showing the Warm up New Zealand Programme would result in $1.2 billion in health savings over 30 years.8 The potential mental health benefits of less traffic congestion,4 less noise pollution,9 and less extreme weather events10 were also mentioned in the Commission’s final advice. The Commission’s final advice also retained evidence estimating the health cost of air pollution at $4.28 billion per year in NZ.11
But the Commission still failed to fully acknowledge the complete spectrum of health co-benefits. Table 1 summarises potential health co-benefits which are discussed or, in some cases, omitted from the Commission’s final advice. The potential health cost-savings from diets less reliant on meat and dairy products were omitted. One NZ modelling study estimated a population shift towards plant-based diets could result in lifetime health gains of 1.0–1.5 million quality-adjusted life-years and health care system cost-savings of $14–20 billion in the population between 2011 and 2121.12 A recent international study recommends this shift is necessary to ensure global life support systems are sustained, while providing a healthy diet to the increasing global population.13
The Commission mentions “behaviour change” over 60 times but never in relation to dietary changes. The Commission states “creating an enabling environment for New Zealanders to make choices that support low-emissions outcomes is critically important,”1, p.248 yet there are no policy recommendations to facilitate behaviour change towards dietary patterns consistent with planetary boundaries.
Reducing water pollution is another area largely omitted from discussion on health co-benefits. The Commission’s final advice states “High levels of nutrient and pathogen loss from pastoral farms can also have human health impacts,”1, p 389 primarily from disease-causing bacteria and nitrate contamination in drinking water. The Commission also links these health impacts to intensive animal farming but fails to provide supporting evidence on the financial costs of these health impacts. A single water-borne outbreak of Campylobacter in Havelock North cost an estimated $21 million14 (as well as causing hospitalisations and deaths). A report prepared by the Law and Economics Consulting Group on behalf of the Ministry of Health in 2010 estimated contaminated drinking water causes 35,000 cases of acute gastrointestinal illness and costs $38.5 million each year.15 Further, nitrate contamination in drinking water has been linked with colorectal cancer and pre-term births.16 The health and financial implications of nitrate contamination could be substantial if additional research reinforces this emerging evidence base.
Table 1. Short summary of the potential costs and cost-savings related to health co-benefits associated with addressing climate change
| Health area | Acknow-ledged in final advice* | Detail as regards health impacts | Economic metrics |
| Extra costs (if no climate change responses) | |||
| Air pollution | Yes | Health costs of air pollution | $4.28 billion (per year)11 |
| Water pollution | No | Cost of acute gastrointestinal illness from this source | $38.5 million (per year)15 |
| Cost-savings (from climate change responses) | |||
| Improved housing | Yes | Health cost-savings from the Warm Up New Zealand programme | $1.2 billion (over 30 years)8 |
| Increased active transport | Yes | Health cost-savings from switching short vehicle trips to walking and cycling | $2.1 billion (lifetime of 2011 cohort) 4 |
| Yes | Health cost-savings from segregating bike lanes from traffic on busy urban roads and slowing traffic on smaller local roads | $13 million (by 2050)5 |
|
| Healthier dietary patterns | No | Health cost-savings from a shift towards plant-based diets | $14-20 billion (lifetime of 2011 cohort)12 |
*But none of these health co-benefits were factored into the GDP modelling by the Commission.
Perhaps the largest missed opportunity in the Commission’s final advice is the exclusion of health co-benefits from the GDP modelling or the narrative around these estimates. The Commission’s explanation for not incorporating health co-benefits into the GDP predictions were: 1) the chosen model cannot include a large amount of technological detail; and 2) the difficulty in fully quantifying these benefits with any accuracy. The model found GDP increases by 0.2-1.0% in 2035 and 0.3-0.7% in 2050 less than it would in the absence of the climate budgets (see Table 2). In absolute terms, the budgets could decrease GDP by a maximum of $45 billion over the next 30 years (given there is no decrease larger than $1 billion until 2035 and the maximum yearly decrease is 3 billion in 2050). In this context, the health costs associated with air pollution ($4.28 billion per year unadjusted for inflation) are almost three times higher than the average yearly GDP deficits until 2050 (~$1.5 billion per year).
While the GDP model’s constraints prevented including health co-benefits, the Commission could have contextualised the GDP estimates using the substantial health co-benefits outlined in Table 1. That is, once accounting for the full spectrum of health co-benefits, it is likely that the projected net deficit in GDP would actually be net positive. That is, society could gain overall from making these responses to climate change. Although GDP is a crude metric – if people are healthier then this means they are typically more productive in their work (further raising GDP). Reduced illness burdens that then lower government expenditure on health services can also potentially raise GDP by diverting excess government funds to infrastructure or education that further increase productivity.
Table 2. GDP projections from the Commission’s C-PLAN modelling ($ billion)*
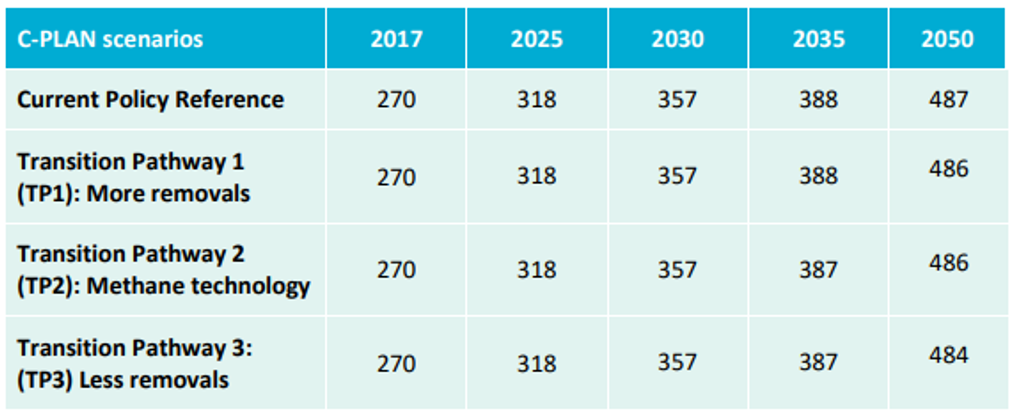
*Table 15.2 from Climate Change Commission’s final advice 1
This blog has focused on highlighting the Commission’s missed opportunity to fully acknowledge the heatlh co-benefits of climate action within the constraints of the Commission’s primary reporting method (eg, GDP modelling). However, we acknowledge an overemphasis on GDP neglects the broader health benefits of a healthy environment and the potential implications for health equity. That is, GDP-centred analyses do not account for the distribution of health and economic benefits across the population. A pathway with less impact on GDP may also exacerbate existing health and social inequites by concentrating resources within priviledged populations in order to maintain the status quo.
Our analysis on the financial benefits of health co-benefits also focuses on the relatively short-term health co-benefits (years to decades). As such, it ignores the society-wide, inter-generatonal benefits of avoiding major climate change impacts in the long-term (decades to centuries). Regardless, the objective of this blog was to highlight that even a conservative, limited and short-term view of the potential health co-benefits could still substantially change the narrative around the financial implications of the Commission’s final advice.
Conclusions
The Commission’s final advice improved the discussion of the potential health co-benefits from its draft advice. However, the final advice still failed to account for key areas of health co-benefits related to a shift towards plant-based diets and reduced water pollution. Crucially, the Commission’s advice has failed to adequately incorporate the substantial financial benefits arising from health co-benefits in its final modelling or discussion around the model’s final GDP predictions. Consequently, there is a major missed opportunity to demonstrate the potential net financial benefit climate action could have for society.
*Author positions
Chambers [tim.chambers@otago.ac.nz], Ball and Cleghorn are Senior Research Fellows; Shaw is an Associate Professor; and Wilson, Hales and Baker are Professors, all at the Department of Public Health at the University of Otago, Wellington.
References
- Climate Change Commission. Ināia tonu nei: A low emissions future for Aotearoa. Wellington (NZL): Climate Change Commission; 2021. Accessed 14 Jun 2021. https://ccc-production-media.s3.ap-southeast-2.amazonaws.com/public/Inaia-tonu-nei-a-low-emissions-future-for-Aotearoa/Inaia-tonu-nei-a-low-emissions-future-for-Aotearoa.pdf.
- He Pou a Rangi – the Climate Change Commission. 2021 Draft Advice for Consultation. Wellington (NZL): He Pou a Rangi – The Climate Change Commission; 2021. Accessed 24 Mar 2021. https://www.climatecommission.govt.nz/get-involved/our-advice-and-evidence/.
- Wilson N, Shaw C, Ball J, Baker M, Hales S, Chambers T. NZ’s Climate Change Commission needs to account for the huge potential health benefits of reducing emissions. Online: The Conversation; 2021. Accessed 14 Jun 2021. https://theconversation.com/nzs-climate-change-commission-needs-to-account-for-the-huge-potential-health-benefits-of-reducing-emissions-156036.
- Mizdrak A, Blakely T, Cleghorn CL, Cobiac LJ. Potential of active transport to improve health, reduce healthcare costs, and reduce greenhouse gas emissions: A modelling study. PLoS ONE. 2019;14(7):e0219316. https://doi.org/10.1371/journal.pone.0219316
- Macmillan A, Connor J, Witten K, Kearns R, Rees D, Woodward A. The societal costs and benefits of commuter bicycling: simulating the effects of specific policies using system dynamics modeling. Environ Health Perspect. 2014;122(4):335-344. https://doi.org/10.1289/ehp.1307250
- Chapman R, Howden-Chapman P, Viggers H, O’Dea D, Kennedy M. Retrofitting houses with insulation: a cost-benefit analysis of a randomised community trial. J Epidemiol Community Health. 2009;63(4):271-277. https://doi.org/10.1136/jech.2007.070037
- Howden-Chapman P, Matheson A, Crane J, Viggers H, Cunningham M, Blakely T et al. Effect of insulating existing houses on health inequality: cluster randomised study in the community. BMJ. 2007;334(7591):460. https://doi.org/10.1136/bmj.39070.573032.80
- Grimes A, Denne T, Howden-Chapman P, Arnold R, Telfar-Barnard L, Young C. Cost benefit analysis of the warm up New Zealand: heat smart programme. Wellington (NZL) 2012. Accessed 24 Mar 2021. https://motu.nz/assets/Documents/our-work/urban-and-regional/housing/Cost-Benefit-Analysis-of-the-Warm-Up-New-Zealand-Heat-Smart-Programme.pdf.
- Hegewald J, Schubert M, Freiberg A, Romero Starke K, Augustin F, Riedel-Heller SG et al. Traffic noise and mental health: A systematic review and meta-analysis. Int J Environ Res Public Health. 2020;17(17). https://doi.org/10.3390/ijerph17176175
- The Royal Australian & New Zealand College of Psychiatrists. Addressing the Mental Health Impacts of Natural Disasters and Climate Change-Related Weather Events. Online: The Royal Australian & New Zealand College of Psychiatrists;2020. Accessed 14 Jun 2021. https://www.ranzcp.org/news-policy/policy-and-advocacy/position-statements/addressing-mental-health-impacts-natural-disasters.
- Kuschel G, Metcalfe J, Wilton E, Hales S, Rolfe K, Woodward A. Updated health and air pollution in New Zealand study, Volume 1: summary report. Wellington (NZL) 2012. Accessed 24 Mar 2021. https://www.mfe.govt.nz/sites/default/files/media/Air/updated-health-and-air-pollution-new-zealand-study-summary-report.pdf.
- Drew J, Cleghorn C, Macmillan A, Mizdrak A. Healthy and climate-friendly eating patterns in the New Zealand context. Environ Health Perspect. 2020;128(1):17007. https://doi.org/10.1289/EHP5996
- Willett W, Rockström J, Loken B, Springmann M, Lang T, Vermeulen S et al. Food in the Anthropocene: the EAT–Lancet Commission on healthy diets from sustainable food systems. Lancet. 2019;393(10170):447-492.
- Department of Internal Affairs. Government inquiry into Havelock North drinking water report of the Havelock North Drinking Water Inquiry: Stage 2. Auckland (NZL) 2017. Accessed 11 Feb 2020. https://www.dia.govt.nz/diawebsite.nsf/Files/Report-Havelock-North-Water-Inquiry-Stage-2/$file/Report-Havelock-North-Water-Inquiry-Stage-2.pdf.
- Moore D, Black M, Valji Y, Tooth R. Cost benefit analysis of raising the quality of New Zealand networked drinking water Wellington (NZL): The Law and Economics Consulting Group 2010. Accessed 14 Jun 2021. https://www.dia.govt.nz/diawebsite.nsf/Files/Havelock-North-Water-Inquiry-Stage-2-core-bundle/$file/CB230.pdf.
- Chambers T, Wilson N, Hales S, Baker M. Nitrate contamination in drinking water and adverse birth outcomes: emerging evidence is concerning for NZ. Online: Public Health Expert Blog; 2021. Accessed 14 Jun 2021. https://blogs.otago.ac.nz/pubhealthexpert/nitrate-contamination-in-drinking-water-and-adverse-birth-outcomes-emerging-evidence-is-concerning-for-nz/.
The whole focus on GDP is, of course, misguided. The aim of public policy (and arguably, economics) should be to maximise wellbeing (roughly, QALYs). Not aggregate production (GDP) – that is only useful in sofar as it contributes to wellbeing, not as an aim in itself. In GDP calculations, longer, healthier lives have no value. Unless they translate to higher production, people are irrelevant. Yet living long, healthy lives is what people value most.
And since GDP estimates maximise a mere instrumental value but ignore what we value most, they should never be used to set priorities in public policy.