Richard Edwards, Jude Ball, Janet Hoek, Andrew Waa*
New Zealand Health Survey (NZHS) data was released in late November. In this blog, we assess whether the substantial reductions in smoking prevalence and increase in e-cigarette (EC) use/vaping observed in last year’s survey have continued. Key findings included:
- The accelerated decline in daily and current smoking prevalence first seen in 2020/21 continued into 2021/22, including among Māori and the most deprived population groups, but not among Pacific peoples.
- The greatest reduction in smoking prevalence since 2011/12 occurred among people aged <35 years with much smaller reductions among people aged ≥55 years.
- The rapid increase in prevalence of EC use seen in 2020/21 continued in 2021/22, with the increase greatest among young people aged <25 years.
We explore implications for the Smokefree Aotearoa goal and legislative and regulatory frameworks for smoking and ECs.

Image by dragana991 from iStock
Introduction
This is the fourth annual blog describing key findings about smoking and e-cigarette (EC) use/vaping from the NZ Health Survey (NZHS).
Previous analyses revealed a steady but unspectacular decrease in smoking prevalence from 2011/12 to 2019/20, though large inequities in smoking by ethnicity and socio-economic status (SES) persisted.
In last year’s blog we reported that the 2020/21 survey indicated substantial increases in quit rates and decreases in smoking prevalence, including among Māori and Pacific peoples and the most deprived population groups. These findings followed steady but unspectacular declines in smoking prevalence from 2011/12 to 2019/20. Nonetheless, large inequities in smoking prevalence persisted in the 2020/21 survey. We also reported that declines in smoking prevalence were concentrated among younger age groups, continuing a long-standing trend. The 2020/21 survey also revealed a large increase in daily and current (at least monthly) EC/vaping prevalence, particularly among young people aged <25 years.
We cautioned about reading too much into one year’s data particularly as the 2020/21 survey was adversely affected by COVID-19 (e.g., the sample size was reduced) and the extraordinary circumstances of the pandemic may have resulted in temporary behaviour changes affecting smoking and vaping. 1 2
This blog provides updated information on patterns and trends in smoking and vaping prevalence from the 2021/22 NZHS data and explores implications for the Smokefree Aotearoa goal and legislative and regulatory frameworks smoking and ECs.
New Zealand Health Survey methods
The NZHS is a rolling nationally representative population survey conducted through face to face computer assisted personal interviews (CAPI) every year since 2011/12. The survey aims to sample around 14,000 adults aged 15 years and over, and usually averages around 13,500 participants. Response rates were around 80% up to 2011/12to 2018/19 before falling slightly to 75% in 2019/20 and 77% in 2020/21. However, data collection has been badly affected by COVID-19 and in 2020/21 the sample size was reduced to 9709 adults and in 2021/22 was only 4,434 adults. In 2021/22, largely due to reduced availability of interviewers, response rates fell to 56% and around a third of interviews were conducted by computer-assisted video interviews (CAVI) rather than face to face.
The smaller 2021/22 sample size reduced the precision of estimates reported and the ability to conduct meaningful sub-group analyses.
Full details of the methods and a methodology report are available on the Ministry of Health website. Data used in the blog are sourced from the NZHS data explorer.
Key findings
1. Overall smoking prevalence and e-cigarette use trends
Figure 1 shows trends in current (at least monthly) and daily smoking and vaping/EC use prevalence among adults (≥15 years) between 2011/12 and 2021/22.
Daily smoking prevalence in 2021/22 was 8.0% (95%CI: 7.0-9.0%) with an estimated 331,000 New Zealanders smoking daily. Current (at least monthly) smoking prevalence was 9.2% (95%CI: 8.1-10.3%), representing around 380,000 people.
Current and daily smoking prevalence declined by about 0.6% per year in absolute terms from 2011/12 to 2019/20. In the two years since 2019/20, there has been a sustained acceleration of the decline in smoking with an absolute fall of 3.6% in daily and 4.5% in current smoking prevalence. This reduction represents an estimated 154,000 fewer people smoking daily and 179,000 fewer smoking monthly or more often, and is similar to the estimated reductions in numbers between 2011/12 and 2019/20 (188,000 and 182,000 respectively).
Use of ECs was first assessed in the 2015/16 NZHS; since then, the prevalence of current and daily EC use has steadily increased. The rate of increase in vaping accelerated between 2019/20 and 2021/22, with current use approximately doubling from 5.3% to 10.3% (95%CI 9.1-11.7%) and daily use increasing from 3.5% to 8.3% (95%CI 7.1-9.7%). These represent an estimated additional 202,000 daily vapers and 213,000 current vapers over the two year period.
The increase in daily and current EC use between 2019/20 and 2021/22 occurred concurrently with the large reduction observed in smoking prevalence (Figure 1), whereas the more gradual increase in EC use between 2015/16 and 2019/20 was not associated with a substantial change in the rate of decline in smoking prevalence. We note in the discussion the contrasting evidence in the NZHS figures about the association between increasing EC use and declines in smoking prevalence, and the need for a more detailed analysis to explore this issue further.
Figure 1 Trends in adult (≥15 years) current (≥ monthly) and daily smoking and e-cigarette use (NZHS 2011/12 to 2021/22)

2. Smoking and e-cigarette use by gender and age
Daily (8.6% men vs 7.3% women) and current (9.9% men vs 8.4% women) smoking prevalence in 2021/22 were slightly higher among men. Since 2019/20, absolute decreases in current and daily smoking prevalence have been similar among men and women. E-cigarette use was also similar among men and women in 2021/22, with current EC use 10.6% for men vs 10.1% for women and daily EC use 8.5% for men vs 8.1% for women.
Figure 2 shows current smoking prevalence by age group from 2019/20 to 2021/22. Due to small numbers, data for smoking among 15-17 year olds were not available in 2021/22 (prevalence in this age group was very low in 2020/21 at 1.4%). Current smoking prevalence in 2021/22 varied between 9.6% and 11.3% for 18-24 years, 25-34 years, 35-44 years and 55-64 years age groups, compared to 5.9% among 65-74 years and 3.3.% for ≥75 years. There were similar patterns in daily smoking prevalence.
Figure 2 Current (≥ monthly) smoking prevalence by age group (NZHS 2019/20-2021/22)
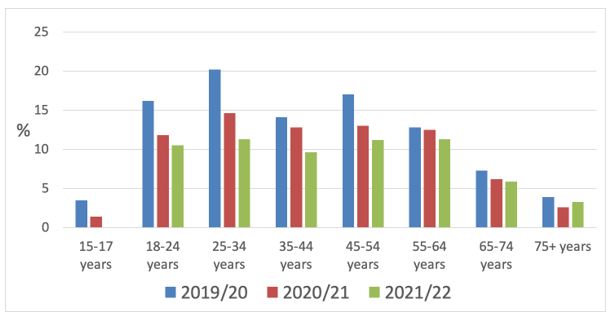
Figures for smoking among 15-17 year olds were not available in 2021/22 due to small sample numbers
Figure 2 suggests that reductions in smoking prevalence since 2019/20 have been greatest in younger age groups.
Figure 3 displays absolute changes in current smoking prevalence by age-group during three time periods since 2011/12. Reductions in smoking prevalence were greatest in absolute terms for the 15-24, 25-34 and 35-44 years age groups during the two periods up to 2019/20 and in age groups between 15-24 years and 45-54 years in the period since 2019/20. Changes in prevalence in age groups above 55 years have been modest during all time periods since 2011.
Figure 3 Changes in current (≥ monthly) smoking prevalence by age group and time period since 2011 (NZHS 2011/12-2021/22)
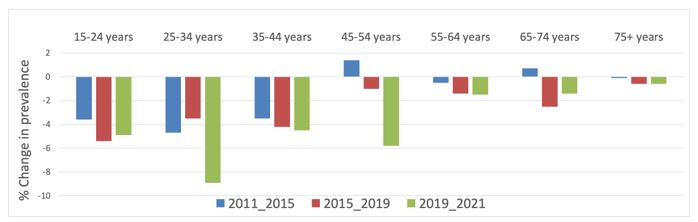
Figure 4 shows patterns of EC use by age from 2019/20 to 2021/22. Vaping has increased rapidly, particularly among younger age groups (although data is not available for 15-17 year olds in 2021/22). In 2021/22 EC use was most prevalent among 18-24 year olds (22.9% daily, 27.8% current) but progressively less prevalent among people aged 25-44 and 45-64 years, and relatively rare among people aged 65 or older.
Figure 4 Daily e-cigarette use by age group (NZHS 2019/20-2021/22)
 Figures for EC use among 15-17 year olds were not available in 2021/22 due to small sample numbers
Figures for EC use among 15-17 year olds were not available in 2021/22 due to small sample numbers
3. Smoking and e-cigarette use among adolescents and young adults
Figure 5 presents trends in current and daily smoking prevalence and EC use among 15-24 year olds since 2011/12.
Current and daily smoking prevalence among 15-24 year olds reduced steadily from 2011/12 to 2019/20 (current and daily smoking declined about 1.1% per annum on average during this period). EC use increased steadily from 2015/16 to 2019/20.
Between 2019/20 and 2020/21 there were very substantial declines in current and daily smoking prevalence, coinciding with a rapid increase in daily and current EC use. The decline in smoking did not continue between 2020/21 and 2021/22, but the rapid increase in EC use continued. EC use is now approximately three times more prevalent than smoking in this age group with almost a quarter (23.8%) of 15-24 year olds using ECs at least monthly and almost a fifth (18.6%) using them daily. Logically, a large proportion of 15-24 year old vapers will be non-smokers.
Data on smoking and EC use among young adults by ethnicity are not available in the NZHS data explorer.
Figure 5 Trends in current (≥ monthly) and daily smoking and e-cigarette use among 15-24 year olds (NZHS 2011/12-2021/21)
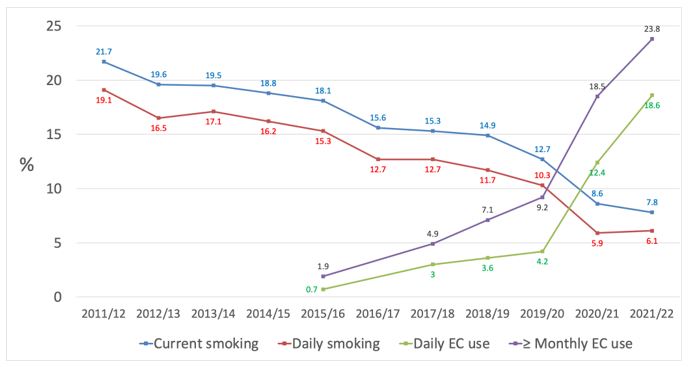
The data presented in Figure 5 suggest some substitution of smoking with EC use has occurred among 15-24 year olds. However, the absolute increase in prevalence of EC use since 2019/20 to 2021/22 was much larger than the reduction in the prevalence of smoking, and therefore the prevalence of use of any nicotine product (cigarettes or ECs) will have increased since 2019/20. For example, daily smoking declined by 4.2% in absolute terms during this period whilst daily EC use increased by 14.4%. This finding also suggests many EC users in this age group were people who would not have begun smoking.
However, it is difficult to quantify the increase in any nicotine product use and the proportion of current vapers who are non-smokers because the NZHS Explorer data does not identify the proportion of people who are dual users. For example, simply adding smoking and EC use prevalence without adjusting for dual use will over-estimate prevalence of any nicotine product use.
4. Smoking and e-cigarette use by ethnicity
Figures 6 and 7 show trends in current and daily smoking prevalence by ethnicity. The substantial decline in Māori current and daily smoking prevalence seen in 2020/21 continued in 2021/22, but the decline in Pacific smoking in 2021/22 was either much less spectacular (current smoking) or partially reversed (daily smoking). Substantial inequities persist, although absolute differences in prevalence narrowed in 2021/22, particularly for Māori compared to European/other.
There was a substantial decline in Māori current smoking prevalence from 31.2% in 2019/20 to 20.9% in 2021/22 (Figure 6). The absolute difference in current smoking prevalence between Māori and European/others narrowed from 19.4% in 2019/20 to 12.4% in 2021/22.
Similarly, Māori daily smoking prevalence declined from 28.6% in 2019/20 to 19.9% in 2021/22 (Figure 7). The absolute difference in daily smoking among Māori compared to European/others narrowed from 18.4% in 2019/20 to 12.7% in 2021/22.
Figure 6 Trends in current (≥ monthly) smoking prevalence by ethnicity (NZHS 2011/12-2020/21)
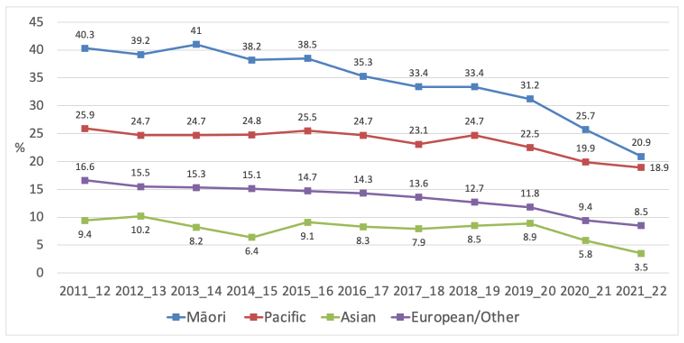
Figure 7 Trends in daily smoking prevalence by ethnicity (NZHS 2011/12-2020/21)

The decrease in smoking was greater among Māori women e.g., current smoking prevalence fell from 35.0% to 20.0% while men showed a smaller decline from 27.3% to 21.8%. This is the first time during the period since 2011/12 that daily and current smoking prevalence has been lower among Māori women than Māori men.
Since 2011/12, Māori smoking prevalence has almost halved with current smoking reducing from 40.3% to 20.9% in 2021/22. The absolute decreases in Māori current and daily smoking prevalence in the two years from 2019/20 to 2021/22 were similar in magnitude to those for the 8-year period from 2011/12 to 2019/20. However, relative differences in prevalence did not change appreciably and Māori remain almost three times more likely than non-Māori to be current smokers in 2021/22 (prevalence ratio: 2.88, 95%CI: 2.28 to 3.64, adjusted for age and gender).
By contrast with Māori, Pacific current smoking prevalence has only reduced by about a quarter from 2011/12 to 2021/22 – from 25.9% to 18.9%. The Pacific sample was relatively small in 2021/22 and changes in current and daily smoking prevalence between 2020/21 and 2021/22 were not statistically significant. However, the changes in Pacific smoking prevalence since 2019/20 were much less dramatic than for Māori. Current smoking prevalence decreased from 22.5% in 2019/20 to 18.9% in 2021/22, but daily smoking prevalence was essentially unchanged. Pacific people were over twice as likely to be current smokers that non-Pacific people in 2021/22 (prevalence ratio: 2.29, 95%CI: 1.55 to 3.39, adjusted for age and gender).
Smoking prevalence among Asian peoples has also declined since 2019/20 and reached 3.5% for current smoking and 2.6% for daily smoking in 2021/22.
There were also differences in EC use by ethnicity (Figure 8), with substantial increases particularly among Māori and Pacific peoples between 2019/20 and 2021/22. The increase in EC use among Māori and Pacific peoples was much greater among women in the 2021/22 survey. For Māori, daily EC use decreased from 15.2% to 13.8% for men but increased from 10.0% to 21.2% for women, while daily use among Pacific men increased from 11.7% to 16.9% and from 6.3% to 16.6% among Pacific women.
Figure 8 Daily e-cigarette use by ethnicity (NZHS 2019/20 – 2021/22)

5. Smoking prevalence and e-cigarette use by socio-economic status
Figure 9 shows there are very large disparities in smoking by SES (as measured by NZDep, an indicator of neighbourhood deprivation).
Figure 9 Trends in current (≥ monthly) smoking prevalence by socioeconomic status (NZDep, NZHS 2011/12-2021/22)
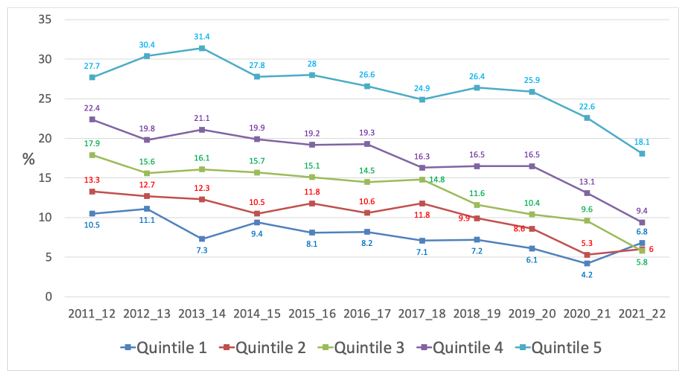
NZDep quintile 1 is the most affluent and quintile 5 the most deprived.
Substantial reductions occurred in current smoking (7.8% and 7.1% absolute reductions) since 2019/20 among the two most deprived quintiles, but much less so among the more affluent quintiles. There were similar patterns in the decline in daily smoking by deprivation level over this period. The reduction in current smoking prevalence in the most deprived quintile since 2019/20 was substantially higher than during the whole of the period from 2011/12 to 2019/20 (7.8% vs 1.8% absolute reduction).
However, although socioeconomic differences in smoking prevalence have narrowed, substantial inequities persist. For example, current smoking prevalence in 2021/22 was about three times higher (prevalence ratio: 2.98, 95%CI: 1.61 to 5.51, adjusted for age, gender and ethnicity) among the most deprived quintile of the population compared to the most affluent quintile. In quintile 5 current smoking prevalence was 18.1% (representing 147,000 people who smoke) compared to 6.8% in quintile 1 (56,000 people). Daily smoking was over four times higher (adjusted prevalence ratio: 4.31, 95%CI: 2.27 to 8.21) in the most deprived quintile, with daily smoking prevalence 17.4% (142,000 people) in quintile 5 compared to 4.8% (39,000 people) in quintile 1.
E-cigarette use also varied with SES (higher in more deprived groups), though less dramatically than for smoking. For example, daily use in 2021/22 was 6.0% (an increase from 2.2% in 2019/20) among NZDep quintile 1 compared with 10.4% in quintile 5 (up from 5.2% in 2019/20). After adjustment for age, gender and ethnic group, differences were minimal (prevalence ratio for quintile 5 vs quintile 1: 1.08 95% CI: 0.62, 1.91) and not statistically significant.
6. Quit rates for smoking
The NZHS estimates smoking quit rates for smoking from the number of people who reported they had quit smoking in the last year and had been quit for at least a month divided by the number of last year quitters plus the number of people who smoke daily. These figures will over-estimate long term quit rates as some recent quitters will subsequently relapse to smoking and self-reported figures may overestimate true quit rates. The quit rates are for quitting smoking, but not necessarily quitting all nicotine product use: some recent quitters will have switched to ECs. The proportion of quitters who have switched to ECs is not available from the data explorer.
Figure 10 shows that overall quit rates were fairly constant (lowest = 9.6% (2015/16), highest = 13.6% (2019/20)) during the period from 2011/12 and 2019/20, but increased markedly to 19.0% in 2020/21 and 20.2% in 2021/22. There were also large increases in quit rates for all ethnic groups after 2019/20; with particularly large increases among Māori (9.4% in 2019/20 vs 20.9% in 2021/22) and Pacific peoples (8.8% vs 27.1%). Quit rates were generally higher among European/other people than among Māori and Pacific peoples from 2011/12 onward, but this was no longer the case in 2021/22.
The high quit rates in 2021/22 among Pacific peoples appears inconsistent with the modest changes in smoking prevalence shown in Figures 6 and 7. However, the numbers of Pacific people and of Pacific people who smoke or have quit in the last year in the NZHS is small so these and previous figures for Pacific quit rates may be affected by chance fluctuations and should be viewed with caution.
Figure 10 Trends in quit rates by ethnicity # (NZHS 2011/12 to 2021/22)

Quit rates among Asian peoples are not reported in this graph as these fluctuated widely, likely reflecting chance variations due to the smaller numbers of participants identifying with Asian ethnicities.
Quit rates also varied substantially by SES (Figure 11) and age-group (Figure 12).
Figure 11 shows that there was a strong socio-economic gradient in quit rates in 2019/20 and 2020/21, but this was less clear cut in 2021/22 (partly because figures were not available for quintile 1 due to small sample size).
Figure 11 Quit rates by socioeconomic status (NZDep, NZHS 2019/20 – 2021/22)
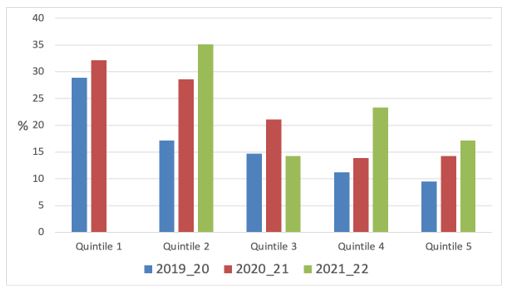
NZDep quintile 1 is the most affluent and quintile 5 the most deprived. Quit rates were not available for quintile 1 in 2021/22 due to small numbers in the sample.
Figure 12 shows that quit rates decrease greatly with age. The age-related quitting gradient appears to have increased since 2019/20 due to larger increases in quit rates among age groups below 55 years.
Figure 12 Quit rates by age group (NZHS 2019/20-2021/22)

Commentary
Key findings from the 2021/22 NZHS include the following:
- The accelerated decline in daily and current smoking prevalence, first seen in 2020/21, continued into 2021/22 and was mirrored by sustained increases in quit rates.
- Māori smoking prevalence continued to fall rapidly in 2021/22 and absolute differences in smoking prevalence from European/others have narrowed, though relative differences persisted.
- Pacific smoking prevalence has declined more slowly since 2011/12 and the decline in prevalence has not accelerated since 2019/20.
- Smoking prevalence in the most deprived population groups has declined substantially since 2019/20 and the absolute and relative difference in smoking compared to more affluent groups has narrowed.
- The greatest reduction in smoking prevalence throughout the 2011/12 to 2021/22 period occurred among people aged <35 years with only small reductions among people aged ≥55 years.
- The rapid increase in prevalence of daily and current EC use seen in 2020/21 continued in 2021/22 with the increase greatest among young people aged <25 years.
Mostly, the smoking trends in the 2021/22 NZHS are very encouraging. The acceleration in the decline in smoking appears to have been maintained, including among Māori (particularly Māori women) and among the most deprived population groups. However, the lack of reduction in Pacific smoking prevalence is a major concern. Evidence that the accelerated decline in smoking prevalence seen in 2020/21 has generally continued means it is less likely that the accelerated decline in prevalence since 2019/20 is due to random fluctuations in year-to-year results. However, it will be reassuring if there are similar findings in future NZHS with full sample sizes that are not conducted in the shadow of a pandemic.
The NZHS is carried out each year using largely consistent methods. The most plausible threat from bias is that the COVID-19 pandemic resulted in a systematic change to the methods (e.g., to the sampling strategy, response rates or to the data collection methods) affecting particularly the 2020/21 and 2021/22 surveys.
In 2020/21, there were no major changes to the data collection methods other than a small number (n=31) of interviews were conducted by video rather than all being face-to-face (as in previous surveys). In 2021/22 about a third of interviews were conducted by video. However, the video interviews replicated the in-person interview as much as possible. The NZHS team (personal communication) also conducted a comparison of results for key indicators by interview type. This suggested that any biases due to change of data collection method were unlikely to be substantial.
There were substantial changes to response and coverage rates and the sample size in 2021/22. This may have introduced greater selection bias (e.g. the degree to which participants in the survey differ in smoking and EC use rates compared to the overall population) and will have reduced precision (increased the width of confidence intervals/margin of error for survey estimates). There is some evidence to suggest an increase in selection bias is unlikely to have greatly affected the findings, though it cannot be ruled out. For example, if the 2020/21 and 2021/22 NZHS participants were systematically different from previous surveys, then substantial changes might be expected in multiple measures included in the survey, particularly in other health-related risk behaviours (such as hazardous and heavy episodic drinking and illicit drug use). However, between 2019/20 and 2020/21, there were no substantial changes in these behaviours, and then small declines in prevalence (e.g. hazardous drinking fell from 19.9% to 18.8% among the adult population) between 2020/21 and 2021/22.
The most plausible explanations for the observed changes in smoking prevalence since 2019/20 are: (i) growing use of ECs is resulting in increased quitting smoking among people who smoke and/or reduced uptake if young people substitute vaping for smoking; (ii) the impact of tobacco control policies and interventions that have been implemented or proposed; (iii) an ongoing effect of the COVID-19 pandemic (e.g., increased quitting through various possible mechanisms).
We discussed the likelihood that the COVID-19 pandemic explained increased declines in smoking prevalence in last year’s blog and concluded these were unlikely to be the main drivers of the decreases observed.
Other tobacco control policies and interventions may have contributed to the observed smoking prevalence declines, but new polices or interventions are probably unlikely to be the main cause for these. New tobacco control policies since 2019/20 have been restricted to an above inflation tobacco excise increase on January 1 2020, some relatively modest changes to mass media campaigns on smoking, and the introduction of legislation prohibiting smoking in cars in November 2021.
However, previous policies could be having an ongoing or enhanced impact. For example, tobacco tax increases and reduced affordability of cigarettes and tobacco may have had an increased effect in the context of economic uncertainty and hardship caused by the pandemic. Supporting evidence comes from the ITC NZ/EASE survey (data collected October 2020 to February 2021) in which 90% of 692 people who smoke stated the price of cigarettes as a reason for wanting to quit (unpublished data) – the commonest reason given. It is also possible that the announcement of potential major new policies in the Smokefree Aotearoa Action Plan consultation document in April 2021 resulted in some anticipatory quitting among people who smoke, although this seems unlikely to have been a major influence.
Accelerated increases in EC use since 2019/20 coincided with more rapid declines in smoking prevalence and provides evidence to support the hypothesis that EC use contributed to recent reductions in smoking prevalence in New Zealand. A more detailed analysis (outside of the scope of this blog) of rates of EC use among recent quitters and of the degree to which smoking prevalence declines mirrored increases in EC use among different population sub-groups and exploration would help evaluate the likely impact of ECs. For example, evidence in support of the hypothesis is that some of the biggest increases in EC use and largest smoking prevalence declines have been among Māori women. However, against the hypothesis is that there have been similarly substantial increases in EC use among Pacific women, but little change in smoking prevalence. More detailed analyses are also required to assess whether EC use has displaced smoking among young people or attracted users who would not have smoked.
So what are the implications for future policy and practice and for the equitable achievement of the Smokefree Aotearoa 2025 goal?
First, the sustained reductions in smoking prevalence, including among Māori, suggest that the smokefree goal is attainable for all peoples in Aotearoa, particularly if the bold measures included in smokefree legislation before Parliament are introduced promptly (with mandated denicotinisation being the most pivotal). However, smoking continues to place a much higher burden on Māori and Pacific peoples. Given the continued inequities in smoking prevalence, ensuring Māori and Pacific governance over and engagement with the implementation of smokefree strategies and actions is essential, as is ongoing evaluation of new measures, particularly their impact on inequities.
Second, the findings of slower declines in smoking prevalence among Pacific peoples (and a possible increase in daily smoking prevalence) and older age groups suggests that greater attention is needed to implementing interventions that are effective among these groups and monitoring the impact of interventions on these populations as the Action Plan is rolled out.
Third, smoking prevalence among 18-24 year olds did not decrease significantly in the 2021/22 survey, despite very high prevalence of EC use in this age group. This underlines the importance of implementing the Smokefree Aotearoa Action Plan measures, which have the potential to greatly reduce smoking uptake smoking among young people.
Fourth, the findings are mostly consistent with the hypothesis that increasing EC use/vaping is contributing to falls in smoking prevalence and achievement of the Smokefree Aotearoa goal, and so are supportive of current legislation and regulations that ensure that people who smoke have ready access to these products. However, more detailed analysis should be undertaken to provide more definitive evidence.
Fifth, the continued rapid increase in EC use and increase in overall use of nicotine products (EC use and smoking prevalence combined) among young people aged < 25 years, many of whom would not have smoked, is worrying. It suggests that current legislation and regulations are failing to protect adolescents and young adults from the risk of starting to vape. Concerns include uncertainties about the long-term health effects of vaping and the risk of creating a new cohort of young people addicted to nicotine. The latter is at odds with the Tupeka Kore vision.
When submitting on the Smokefree Environments and Regulated Products (Smoked Tobacco) Amendment Bill, we called for a review of how vaping and other nicotine products are regulated. We continue to call for such a review, which should assess how regulations can best balance the interests of people who smoke and could benefit from switching to ECs and those of young people who do not smoke and will not benefit from commencing EC use. The findings of the 2021/22 NZHS underline the urgency and importance of carrying out that review.
* Author details: All authors are with ASPIRE2025 and the Department of Public Heath, University of Otago, Wellington
References
- Chun HR, Cheon E, Hwang JE. Systematic review of changed smoking behaviour, smoking cessation and psychological states of smokers according to cigarette type during the COVID-19 pandemic. BMJ Open 2022;12(6):e055179. doi: 10.1136/bmjopen-2021-055179 [published Online First: 2022/06/15]
- Gendall P, Hoek J, Stanley J, et al. Changes in Tobacco Use During the 2020 COVID-19 Lockdown in New Zealand. Nicotine Tob Res 2021;23(5):866-71. doi: 10.1093/ntr/ntaa257 [published Online First: 2021/01/31]
]]>