
Associate Professor Nick Wilson, Professor Tony Blakely
 A recently published review has quantified the estimated benefits and harms of taking regular aspirin for disease prevention. The results indicate a relatively favourable benefit-to-harm ratio (good for preventing various cancers and heart attacks – but also harmful in terms of causing gastric bleeding and one type of stroke). But for some people, the relative size of the benefit may still not be enough to outweigh the dislike of taking daily medication. This blog briefly looks at the issues and considers possible responses by NZ health agencies and research funders.
A recently published review has quantified the estimated benefits and harms of taking regular aspirin for disease prevention. The results indicate a relatively favourable benefit-to-harm ratio (good for preventing various cancers and heart attacks – but also harmful in terms of causing gastric bleeding and one type of stroke). But for some people, the relative size of the benefit may still not be enough to outweigh the dislike of taking daily medication. This blog briefly looks at the issues and considers possible responses by NZ health agencies and research funders.
What is the evidence?
The evidence that regular low-dose aspirin has cancer prevention benefits has been growing for some years now – and this newly published review article by Cuzick and colleagues provides a state-of-the-art summary and integration of the data. Out of the various cancers, the evidence for colorectal cancer prevention seems the strongest (and comes from two randomised control trials [RCT], two cohort studies and a case-control study). For oesophageal cancer there is also RCT level evidence and for stomach cancer it is based largely on cohort studies. The evidence for other cancers is weaker but is still somewhat suggestive of a benefit from aspirin (e.g., for cancer of the lung, prostate and breast).
There is also evidence around aspirin for primary prevention of cardiovascular disease (but also bleeding risk). According to a review by the US Preventive Services Task Force: “Aspirin reduces the risk of myocardial infarctions in men and strokes in women. The risk of serious bleeding is increased with aspirin use.” Regarding the latter – there seems little doubt that aspirin increases the risk of haemorrhagic stroke and gastrointestinal bleeding (especially over the age of 70 years).
What seems to be the net benefit?
The authors of this new review (Cuzick et al) nicely integrate an assessment of all the benefits and harms. However their summary figure of benefits and harms is still fairly complicated and so a further simplification has been done for this blog (see the Figure below). This figure indicates that the benefits of avoided deaths is around 9 times greater than the deaths caused by aspirin for men (it is about 8 times for women). Another way of framing the issue is in terms of numbers needed to treat to save one life by taking aspirin – which is around 70 men taking aspirin for 20 years from age 55 (using the data in Figure 1). If these lives are typically saved half way through this 20 year period, then the average man taking aspirin will get an extra 52 days of life (undiscounted) prior to reaching age 75 years. This is a fairly good value for money given the cost of aspirin (typically 15 cents or less per tablet at the supermarket) – which equates to $3,800 per life-year gained (undiscounted). But such an analysis is extremely simplistic and a more sophisticated one is needed that would consider many other issues (e.g., lower healthcare costs from disease prevention). A more rigorous analysis would also include the benefit in terms of all non-fatal events prevented (e.g., preventing hospitalisations for non-fatal cancers and for non-fatal heart attacks).
Figure 1: Cumulative effects of aspirin taken for 10 years starting at age 55 years on deaths over the next 20 years (in 100 average-risk men – results summarised from the more complex figure shown in Cuzick et al and the data in their Table 5)
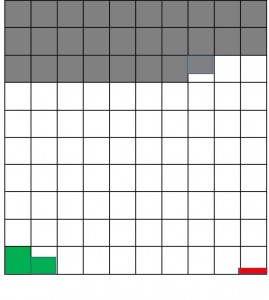 Grey squares at the top – 27.7 deaths unrelated to aspirin by age 75
Grey squares at the top – 27.7 deaths unrelated to aspirin by age 75
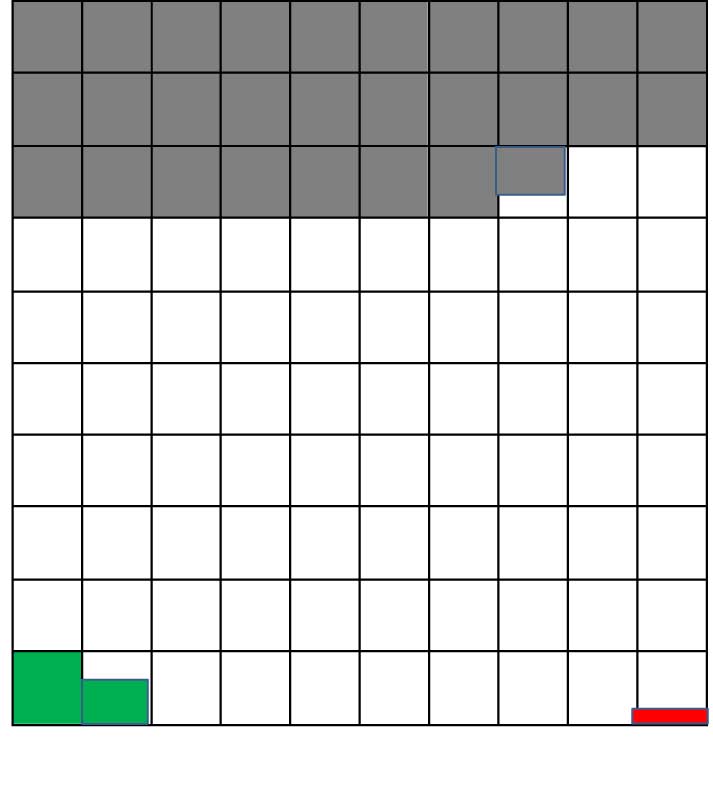
White squares – still alive by age 75 years
Green squares (bottom left) – 1.60 deaths prevented by aspirin by age 75
Red squares (bottom right) – 0.17 deaths caused by aspirin by age 75
What might NZ health agencies do now?
A possible first step is for a suitable NZ health agency (Pharmac, the Ministry of Health, or the National Health Committee) to study the cost-effectiveness of daily aspirin in the NZ setting and for different (age/sex/ethnic) groups. This work could then feed into new guidelines for NZ health workers (for prescribing and for making recommendations to patients). Given the potential role of aspirin in colorectal cancer prevention – a cost-effectiveness analysis could compare the benefits of daily aspirin relative to regular screening for this cancer. It could also make comparisons with other prevention strategies (eating more fruit and vegetables and increasing physical activity).
This process could also help identify if the following options were worthwhile:
- Allowing very long-term prescriptions of low-dose aspirin e.g., for 12-month periods. This might help ensure better uptake by Māori and low-income New Zealanders – to help ensure that health inequalities are addressed.
- For Pharmac to work with suppliers to even further lower the price of low-dose aspirin in supermarkets (though prices are already fairly low as noted above).
- For Pharmac to consider supporting work on the inclusion of aspirin in some types of polypills for the NZ market (e.g., along with blood pressure lowering drugs and a statin in the same pill). We note that NZ researchers have been involved in a range of polypill related research for cardiovascular disease prevention (e.g., for some recent studies: Selak et al in 2014, Selak et al in 2013, Bryant et al in 2013, Elley et al in 2012). In one of these studies, potentially eligible Māori were more likely than non-Māori to proceed to subsequent stages of recruitment for use of a polypill in a trial.
How might NZ research funding agencies help?
Research funders could encourage research that addresses such issues as:
- What are the risks and benefits at older ages for the NZ population (the ASPREE trial in the US and Australia should help inform this issue).
- How might other approaches be used to further lower the risk of gastric bleeding in those taking aspirin (e.g., use of proton pump inhibitors – including combined tablets).
- Can we make use of NZ primary and secondary care data to better understand the timing of the fatal and non-fatal effects relative to when aspirin is started/stopped?
- What is the acceptability of daily preventive medication for New Zealanders? Indeed one recent UK study reported that the general public would only take a daily tablet for disease prevention if it gave them an extra six months or more of life (this was the median result – with a very large variation). This issue of “medication disutility” appears to be inadequately studied and could be considered in future NZ-specific cost-effectiveness analyses around aspirin.
- Is there a problem with daily aspirin in that some individuals might be less likely to perform other daily activities that enhance chronic disease prevention such as a healthy diet, physical activity and quitting smoking?
Clearly daily low-dose aspirin shows a lot of promise for cost-effective disease prevention. But NZ needs careful guideline development and more NZ specific research.
Acknowledgements: The authors thank Dr Linda Cobiac for helpful comments on the draft blog post. The authors have no competing interests (and specificially no links with the pharmaceutical industry).
At the local launch of the World Alzheimer Report 2014 on Wednesday 17 September, low-dose aspirin was discussed by Professor Mark Weatherall as a useful measure that seems to reduce the likelihood of experience the sorts of stroke that are associated with dementia. This seems another spoke to the wheel of possibility when evaluating the potential importance of daily low-dose aspirin from mid-life. here’s a link to the report:
http://www.alzheimers.org.nz/files/alzheimersnews/World-Alzheimer-Report-2014-web.pdf